Tuberculosis agents
Infectious Disease -ALL Agents (INDEX)
![]()
| WARNINGS: See Full Prescribing Information for complete boxed warning. An increased risk of death was seen in the SIRTURO treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81, 2.5%) in one placebo-controlled trial. Only use SIRTURO when an effective treatment regimen cannot otherwise be provided. QT prolongation can occur with SIRTURO. Use with drugs that prolong the QT interval may cause additive QT prolongation. Drug UPDATE: SIRTURO ® (bedaquiline) tablets, for oral use Mechanism of Action:SIRTURO is a diarylquinoline antimycobacterial drug that inhibits mycobacterial ATP (adenosine 5'-triphosphate) synthase, by binding to subunit c of the enzyme that is essential for the generation of energy in M. tuberculosis. INDICATIONS AND USAGE This indication is approved under accelerated approval based on time to sputum culture conversion. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. (1, 14) Limitations of Use: Do not use SIRTURO for the treatment of latent, extra-pulmonary or drug-sensitive tuberculosis or for the treatment of infections caused by non-tuberculous mycobacteria (1). Safety and efficacy of SIRTURO in HIV-infected patients with MDR-TB have not been established, as clinical data are limited (14). DOSAGE AND ADMINISTRATION Prior to administration, obtain ECG, liver enzymes and electrolytes. Obtain susceptibility information for the background regimen against Mycobacterium tuberculosis isolate if possible. (2.2) Only use SIRTURO in combination with at least 3 other drugs to which the patient's MDR-TB isolate has been shown to be susceptible in vitro. If in vitro testing results are unavailable, may initiate SIRTURO in combination with at least 4 other drugs to which patient's MDR-TB isolate is likely to be susceptible (2.3) Recommended dosage: 400 mg once daily for 2 weeks followed by 200 mg 3 times per week (with at least 48 hours between doses) for 22 weeks (2.3) Swallow SIRTURO tablets whole with water and take with food. (2.3) DOSAGE FORMS AND STRENGTHS CONTRAINDICATIONS WARNINGS AND PRECAUTIONS -Discontinue SIRTURO if significant ventricular arrhythmia or a QTcF interval > 500 ms develops. -Use with drugs that prolong the QT interval may cause additive QT prolongation. Monitor ECGs more frequently. -Hepatic-related adverse drug reactions have been reported with use of SIRTURO. Monitor liver-related laboratory tests. -Non-adherence to the treatment regimen could result in failure or resistance. |
| CLINICAL PHARMACOLOGY Ethambutol hydrochloride tablets following a single oral dose of 25 mg/kg of body weight, attains a peak of 2 to 5 mcg/mL in serum 2 to 4 hours after administration. When the drug is administered daily for longer periods of time at this dose, serum levels are similar. The serum level of ethambutol hydrochloride falls to undetectable levels by 24 hours after the last dose except in some patients with abnormal renal function. The intercellular concentrations of erythrocytes reach peak values approximately twice those of plasma and maintain this ratio throughout the 24 hours. During the 24-hour period following oral administration of ethambutol hydrochloride tablets approximately 50 percent of the initial dose is excreted unchanged in the urine, while an additional 8 to 15 percent appears in the form of metabolites. The main path of metabolism appears to be an initial oxidation of the alcohol to an aldehydic intermediate, followed by conversion to a dicarboxylic acid. From 20 to 22 percent of the initial dose is excreted in the feces as unchanged drug. No drug accumulation has been observed with consecutive single daily doses of 25 mg/kg in patients with normal kidney function, although marked accumulation has been demonstrated in patients with renal insufficiency. Ethambutol hydrochloride diffuses into actively growing Mycobacterium cells such as tubercle bacilli. Ethambutol hydrochloride tablets appear to inhibit the synthesis of one or more metabolites, thus causing impairment of cell metabolism, arrest of multiplication, and cell death. No cross resistance with other available antimycobacterial agents has been demonstrated. Ethambutol hydrochloride tablets have been shown to be effective against strains of Mycobacterium tuberculosis but do not seem to be active against fungi, viruses, or other bacteria. Mycobacterium tuberculosis strains previously unexposed to ethambutol hydrochloride have been uniformly sensitive to concentrations of 8 or less mcg/mL, depending on the nature of the culture media. When ethambutol hydrochloride tablets have been used alone for treatment of tuberculosis, tubercle bacilli from these patients have developed resistance to ethambutol hydrochloride by in vitro susceptibility tests; the development of resistance has been unpredictable and appears to occur in a step-like manner. No cross resistance between ethambutol hydrochloride tablets and other antituberculous drugs has been reported. Ethambutol hydrochloride tablets have reduced the incidence of the emergence of mycobacterial resistance to isoniazid when both drugs have been used concurrently. An agar diffusion microbiologic assay, based upon inhibition of Mycobacterium smegmatis (ATCC 607) may be used to determine concentrations of ethambutol hydrochloride in serum and urines INDICATIONS AND USAGE Ethambutol Hydrochloride Tablets plus isoniazid CONTRAINDICATIONS ------------------------------------------------- Children: Adults (suggested doses by lean body weight): Twice weekly directly observed therapy (DOT): 50 mg/kg Three times/week DOT: 25-30 mg/kg (maximum: 2.5 g) Disseminated Mycobacterium avium complex (MAC) in patients with advanced HIV infection: 15 mg/kg ethambutol in combination with azithromycin 600 mg daily Dosing interval in renal impairment: ------------------------------------------------- Supplied: |
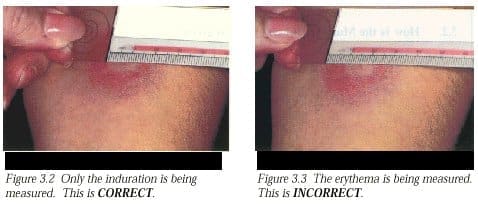
| Mechanism of Action: Isoniazid inhibits the synthesis of mycoloic acids, an essential component of the bacterial cell wall. At therapeutic levels isoniazid is bacteriocidal against actively growing intracellular and extracellular Mycobacterium tuberculosis organisms. Isoniazid resistant Mycobacterium tuberculosis bacilli develop rapidly when isoniazid monotherapy is administered. INDICATIONS AND USAGE: Isoniazid is recommended as preventive therapy for the following groups, regardless of age. (Note: the criterion for a positive reaction to a skin test (in millimeters of induration) for each group is given in parenthesis): 1. Persons with human immunodeficiency virus (HIV) infection (≥ 5 mm) and persons with risk factors for HIV infection whose HIV infection status is unknown but who are suspected of having HIV infection. Preventive therapy may be considered for HIV infected persons who are tuberculin-negative but belong to groups in which the prevalence of tuberculosis infection is high. Candidates for preventive therapy who have HIV infection should have a minimum of 12 months of therapy. 2. Close contacts of persons with newly diagnosed infectious tuberculosis (≥ 5 mm). In addition, tuberculin-negative (< 5 mm) children and adolescents who have been close contacts of infectious persons within the past 3 months are candidates for preventive therapy until a repeat tuberculin skin test is done 12 weeks after contact with the infectious source. If the repeat skin test is positive (> 5 mm), therapy should be continued. 3. Recent converters, as indicated by a tuberculin skin test (≥ 10 mm increase within a 2-year period for those < 35 years old; ≥ 15 mm increase for those ≥ 35 years of age). All infants and children younger than 4 years of age with a > 10 mm skin test are included in this category. 4. Persons with abnormal chest radiographs that show fibrotic lesions likely to represent old healed tuberculosis ( ≥ 5 mm). Candidates for preventive therapy who have fibrotic pulmonary lesions consistent with healed tuberculosis or who have pulmonary silicosis should have 12 months of isoniazid or 4 months of isoniazid and rifampin, concomitantly. 5. Intravenous drug users known to be HIVseronegative ( > 10 mm). 6. Persons with the following medical conditions that have been reported to increase the risk of tuberculosis ( ≥ 10 mm): silicosis; diabetes mellitus; prolonged therapy with adrenocorticosteroids; immunosuppressive therapy; some hematologic and reticuloendothelial diseases, such as leukemia or Hodgkin’s disease; end-stage renal disease; clinical situations associated with substantial rapid weight loss or chronic undernutrition (including: intestinal bypass surgery for obesity, the postgastrectomy state (with or without weight loss), chronic peptic ulcer disease, chronic malabsorption syndromes, and carcinomas of the oropharynx and upper gastrointestinal tract that prevent adequate nutritional intake). Candidates for preventive therapy who have fibrotic pulmonary lesions consistent with healed tuberculosis or who have pulmonary silicosis should have 12 months of isoniazid or 4 months of isoniazid and rifampin, concomitantly. Additionally, in the absence of any of the above risk factors, persons under the age of 35 with a tuberculin skin test reaction of 10 mm or more are also appropriate candidates for preventive therapy if they are a member of any of the following high-incidence groups: 1. Foreign-born persons from high-prevalence countries who never received BCG vaccine. 2. Medically underserved low-income populations, including high-risk racial or ethnic minority populations, especially blacks, Hispanics, and Native Americans. 3. Residents of facilities for long-term care (e.g., correctional institutions, nursing homes, and mental institutions). Children who are less than 4 years old are candidates for isoniazid preventive therapy if they have > 10 mm induration from a PPD Mantoux tuberculin skin test. Finally, persons under the age of 35 who a) have none of the above risk factors (1-6); b) belong to none of the high-incidence groups; and c) have a tuberculin skin test reaction of 15 mm or more, are appropriate candidates for preventive therapy. The risk of hepatitis must be weighed against the risk of tuberculosis in positive tuberculin reactors over the age of 35. However, the use of isoniazid is recommended for those with the additional risk factors listed above (1-6) and on an individual basis in situations where there is likelihood of serious consequences to contacts who may become infected. CONTRAINDICATIONS: --------------------------------------------------- Dosing: Infants and Children: Treatment of active TB infection: Adults: Treatment of active TB infection (drug susceptible): Twice weekly directly observed therapy (DOT): 15 mg/kg (maximum: 900 mg); 3 times/week therapy: 15 mg/kg (maximum: 900 mg) Note: Treatment may be defined by the number of doses administered (eg, "six-month" therapy involves 192 doses of INH and rifampin, and 56 doses of pyrazinamide). Six months is the shortest interval of time over which these doses may be administered, assuming no interruption of therapy. Note: Concomitant administration of 6-50 mg/day pyridoxine is recommended in malnourished patients or those prone to neuropathy (eg, alcoholics, diabetics) Peritoneal dialysis, continuous r venovenous hemofiltration: Dose for Clcr<10 mL/minute Dosing adjustment in hepatic impairment: |
| Pyrazinamide may be bacteriostatic or bactericidal against Mycobacterium tuberculosis depending on the concentration of the drug attained at the site of infection. The mechanism of action is unknown. In vitro and in vivo the drug is active only at a slightly acidic pH.
INDICATIONS AND USAGE: (Patients with drug-resistant disease should be treated with regimens individualized to their situation. Pyrazinamide frequently will be an important component of such therapy.) (In patients with concomitant HIV infection, the physician should be aware of current recommendation of CDC. It is possible these patients may require a longer course of treatment) It is also indicated after treatment failure with other primary drugs in any form of active tuberculosis. Pyrazinamide should only be used in conjunction with other effective antituberculous agents. *See recommendations of Center for Disease Control (CDC) and American Thoracic Society for complete regimen and dosage recommendations. CONTRAINDICATIONS: with severe hepatic damage. WARNINGS: Pyrazinamide should be discontinued and not be resumed if signs of hepatocellular damage or hyperuricemia accompanied by an acute gouty arthritis appear --------------------------------- Children: Twice weekly directly observed therapy (DOT): 50 mg/kg/dose (maximum: 4 g/dose) Adults (dosing is based on lean body weight): Daily therapy: 15-30 mg/kg/day Twice weekly directly observed therapy (DOT): 50 mg/kg Three times/week DOT: 25-30 mg/kg (maximum: 2.5 g) Elderly: Start with a lower daily dose (15 mg/kg) and increase as tolerated. --------------------------------- Avoid use in hemo- and peritoneal dialysis as well as continuous arteriovenous or venovenous hemofiltration. Dosing adjustment in hepatic impairment: Reduce dose |
| Mechanism of Action Rifabutin inhibits DNA-dependent RNA polymerase in susceptible strains of Escherichia coli and Bacillus subtilis but not in mammalian cells. In resistant strains of E. coli, rifabutin, like rifampin, did not inhibit this enzyme. It is not known whether rifabutin inhibits DNA-dependent RNA polymerase in Mycobacterium avium or in M. intracellulare which comprise M. avium complex (MAC). INDICATIONS AND USAGE CONTRAINDICATIONS --------------------------------- Treatment (unlabeled use): Patients not receiving NNRTIs or protease inhibitors: Initial phase (2 weeks to 2 months): 10-20 mg/kg daily (maximum: 300 mg). Adults: Treatment (unlabeled use): Patients receiving nelfinavir, amprenavir, indinavir: Reduce dose to 150 mg/day; no change in dose if administered twice weekly Dosage adjustment in renal impairment: Clcr<30 mL/minute: Reduce dose by 50% --------------------------------- Supplied: |
| [Management of active tuberculosis.]
Dosing (Adults): 2 capsules orally once daily. Supplied: |
| Microbiology Rifampin inhibits DNA-dependent RNA polymerase activity in susceptible cells. Specifically, it interacts with bacterial RNA polymerase but does not inhibit the mammalian enzyme. Rifampin at therapeutic levels has demonstrated bactericidal activity against both intracellular and extracellular Mycobacterium tuberculosis organisms. Organisms resistant to rifampin are likely to be resistant to other rifamycins. Rifampin has bactericidal activity against slow and intermittently growing M tuberculosis organisms. It also has significant activity against Neisseria meningitidis isolates. Infants and Children <12 years: Twice weekly directly observed therapy (DOT): 10-20 mg/kg (maximum: 600 mg) Adults: Twice weekly directly observed therapy (DOT): 10 mg/kg (maximum: 600 mg); 3 times/week: 10 mg/kg (maximum: 600 mg) Latent tuberculosis infection (LTBI): As an alternative to isoniazid: Children: 10-20 mg/kg/day (maximum: 600 mg/day) for 6 months Adults: 10 mg/kg/day (maximum: 600 mg/day) for 4 months. Note: Combination with pyrazinamide should not generally be offered ( MMWR , Aug 8, 2003). H. influenzae prophylaxis (unlabeled use): Infants and Children: 20 mg/kg/day every 24 hours for 4 days, not to exceed 600 mg/dose Adults: 600 mg every 24 hours for 4 days Meningococcal meningitis prophylaxis: Nasal carriers of Staphylococcus aureus (unlabeled use): Adults: 600 mg/day for 5-10 days in combination with other antibiotics Synergy for Staphylococcus aureus infections (unlabeled use): Adults: 300-600 mg twice daily with other antibiotics Hemodialysis or peritoneal dialysis: Plasma rifampin concentrations are not significantly affected by hemodialysis or peritoneal dialysis. Supplied: |
| Mechanism of Action
Rifapentine, a cyclopentyl rifamycin, inhibits DNA-dependent RNA polymerase in susceptible strains of Mycobacterium tuberculosis but not in mammalian cells. At therapeutic levels, rifapentine exhibits bactericidal activity against both intracellular and extracellular M. tuberculosis organisms. Both rifapentine and the 25-desacetyl metabolite accumulate in human monocyte-derived macrophages with intracellular/extracellular ratios of approximately 24:1 and 7:1, respectively. In Vitro Activity Rifapentine and its 25-desacetyl metabolite have demonstrated in vitro activity against rifamycin-susceptible strains of Mycobacterium tuberculosis including cidal activity against phagocytized M. tuberculosis organisms grown in activated human macrophages. The correlation between rifapentine MICs and clinical cure has not been established. Interpretive criteria/breakpoints to determine whether clinical isolates of M. tuberculosis are susceptible or resistant to rifapentine have not been established. In Vivo Activity In mouse infection studies a therapeutic effect, in terms of enhanced survival time or reduction of organ bioburden, has been observed in M. tuberculosis-infected animals treated with various intermittent rifapentine containing regimens. Animal studies have shown that the activity of rifapentine is influenced by dose and frequency of administration ------------------------------------------------------- Intensive phase (initial 2 months) of short-term therapy: 600 mg (four 150 mg tablets) given twice weekly (with an interval of not less than 72 hours between doses); following the intensive phase, treatment should continue with rifapentine 600 mg once weekly for 4 months in combination with INH or appropriate agent for susceptible organisms |
| Management of active tuberculosis: Dosing: Adults: Oral: Patients weighing: </= 44 kg: 4 tablets 45-54 kg: 5 tablets >/= 55 kg: 6 tablets Doses should be administered in a single daily dose. |
National Institutes of Health, U.S. National Library of Medicine, DailyMed Database.
Provides access to the latest drug monographs submitted to the Food and Drug Administration (FDA). Please review the latest applicable package insert for additional information and possible updates. A local search option of this data can be found here.