| Rough estimates (Ideally, drug dosing should be based on more complex pharmacokinetic calculations based on patient specific parameters.)
Conventional dosing:
(Administer usual dose at indicated frequency.)
[CRCL >60 ml/min]: Give q8h.
[40-60]: Give q12h.
[20-40]: Give q24h.
[10-20]: Give q48h.
[<10 ]: Give q48 - 72h.
High-dose (once daily) therapy:
[CRCL >60 ml/min]: Usual dose.
[<60]: Extend interval based on serum level determinations.
Administration for Patients with Impaired Renal Function
Whenever possible, serum tobramycin concentrations should be monitored during therapy.
Following a loading dose of 1 mg/kg, subsequent dosage in these patients must be adjusted, either with reduced doses administered at 8-hour intervals or with normal doses given at prolonged intervals. Both of these methods are suggested as guides to be used when serum levels of tobramycin cannot be measured directly. They are based on either the creatinine clearance level or the serum creatinine of the patient, because these values correlate with the half-life of tobramycin. The dosage schedules derived from either method should be used in conjunction with careful clinical and laboratory observations of the patient and should be modified as necessary. Neither method should be used when dialysis is being performed.
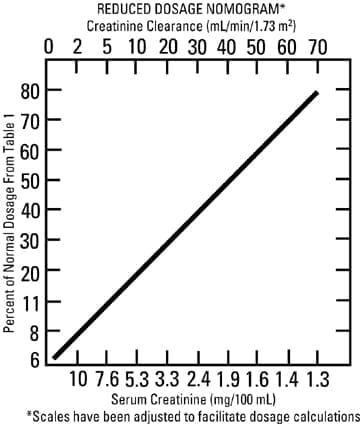
Reduced dosage at 8-hour intervals
When the creatinine clearance rate is 70 mL or less per minute or when the serum creatinine value is known, the amount of the reduced dose can be determined by multiplying the normal dose from Table 1 by the percent of normal dose from the accompanying nomogram.
An alternate rough guide for determining reduced dosage at 8-hour intervals (for patients whose steady-state serum creatinine values are known) is to divide the normally recommended dose by the patient’s serum creatinine.
Normal dosage at prolonged intervals
If the creatinine clearance rate is not available and the patient’s condition is stable, a dosage frequency in hours for the dosage given in Table 1 can be determined by multiplying the patient’s serum creatinine by 6.
Alternatively: Dosing interval in renal impairment: I.M., I.V.:
Conventional dosing:
Clcr 60 mL/minute: Administer every 8 hours
Clcr 40-60 mL/minute: Administer every 12 hours
Clcr 20-40 mL/minute: Administer every 24 hours
Clcr 10-20 mL/minute: Administer every 48 hours
Clcr<10 mL/minute: Administer every 72 hours
High-dose therapy: Interval may be extended (eg, every 48 hours) in patients with moderate renal impairment (Clcr 30-59 mL/minute) and/or adjusted based on serum level determinations.
Hemodialysis: Dialyzable; 30% removal of aminoglycosides occurs during 4 hours of HD - administer dose after dialysis and follow levels |


